Healthcare is the only place where I see people fighting on how to code something in order to get paid. How does that make sense when the healthcare provider can not understand how to code something so the Insurance company pays for it. Why would somebody need a degree on how to factually code something for the insurance company? It is all designed to keep things complicated so that they can get more money from the patient.
2 Likes
Before 1980 there were indemnity policies with almost no paperwork. Doctor and nurse wrote whatever down and it was paid. Then with computers HMOs could chop up every bit of treatment into a pay decision.
Insurers like to raise payouts to doctors and pharma because they get a percentage of a yearly rising premium that has to cover the rising costs.
The coding is cross referencing the individual procedures. A doctor should not bill out to do that. Getting in a coding specialist reduces costs.
The problem is not really the doctors or pharma. The problem is the population is about ten years older on average.
Insurers since the HMOs came on the scene have reduced the insured pool of people. That is another problem. Some of that is jobs that do not have much or any insurance as a benefit.
The entire thing is the dog chasing his tail. Unlike the dog none of us are happy about it. Unless the proverbial dog is the insurance company.
1 Like
If that were true you wouldn’t have insurers like Humana, constantly refusing to pay for procedures as their first line of defense. Also you wouldn’t have them fighting with coding specialists.
My sister works for a major hospital as a coding specialist. She has a masters degree. While she saves the hospital money by getting the most out of the billing, I am saying it is ridiculous. It is a waste of resources. It shouldn’t take someone with a Masters degree to figure out the billing and still have to fight over the billing. It shows you exactly what is going on when a hospital and insurer are fight over the billing. It should only take a secretary, going through a book on billing, and choose the correct code. Easy peasy but that is not what they want. That is also why you can’t get hospitals to tell you exactly what the cost is for an operation. It’s all fuzzy math.
2 Likes
A friend is a nurse, working in administration in a major hospital group, as basically a ‘fixer’. If there’s a problem, she is often called to come check it out and ‘fix it’.
She is on hiring committees, and hires for all kinds of positions, including coding.
Just this past weekend, she and I were talking about coding jobs, cause one of her kids has decided to try coding.
She says that starting pay is about 18-20$/hr.
There are two branches:
One branch is coding FOR the hospital/provider. The coder is responsible for getting the hospital paid.
The other branch is coding for the INSURANCE company - to DENY payment.
A ‘good’ coder masters ONE of the branches, WFH, and can job hop for better pay.
A GREAT coder master’s BOTH branches, knows the correct codes for both getting payment, and for denying coverage, and can effectively troubleshoot a claim to see how to ‘fix’ it.
Therefore, a great coder can demand Excellent pay. I don’t remember her saying what is ‘excellent’.
She said coding requires the ability to FOCUS, and attention to detail.
I attended a coding class for a few weeks, back in the day. I wasn’t interested in being a coder, I just wanted to know how it worked, and the class was ‘free’ to me.
It seems to me to be a ‘skill/job’ that is ripe for AI disruption.
FWIW
![]()
ralph
3 Likes
I agree Ralph but just so people do not get confused. The coder we are talking about is someone who decides the billing for Insurance purposes, not a software coder that writes software code like Java. A masters degree in billing coder can pay over 110,000 a year.
1 Like
Sure you would. They place a percentage on top of all costs to make a profit. The insurers place a profit margin on their administration costs.
Absolutely true it is a waste of resources. I like your grasp of the obvious. LOL
I like your ability to argue with people that have a better understanding than yourself and still show your utter incompetence. LOL
There’s a fine line between, “getting the most out of the billing” and Medicare fraud. FL Senator Rick Scott was CEO of a for-profit hospital operator convicted of the then world record Medicare fraud.
intercst
3 Likes
My family has been for socialized medicine since 1907. I think I was in the cradle when it was first explained to me.
In the meantime you can take a joke.
That is some great advice. ![]()
1 Like
There are 4 parts of the condition based monitoring process:
- Collect data (install sensor or collect data from test)
- Compare the data to benchmarks
- Analyze the data (including other semantic data) to diagnose or disposition
- Execute the plan
Providing CGM data (or any other) without continuity in all 3 primary steps is generally useless.
Step 3 is the most valuable of the 4 steps.
1 Like
While this is true, and no doctor will sift through all the data all the time. However, when the doctor is looking for something wrong, they might sift through the relevant data.
In my case, my doctor (PCP) literally handed me sheets of paper with 4 columns and 31 rows on it - columns were “date”, “morning”, “afternoon”, “evening/night”, and asked me to take my BP and record it 3 times a day, then when I returned for my followup appointment, I gave him the sheets of paper with my handwritten, manually taken BP measurements on it. I suspect it would be A LOT easier for my Apple health app to “beam” the data right into his system via this newfangled thing called the Internet.
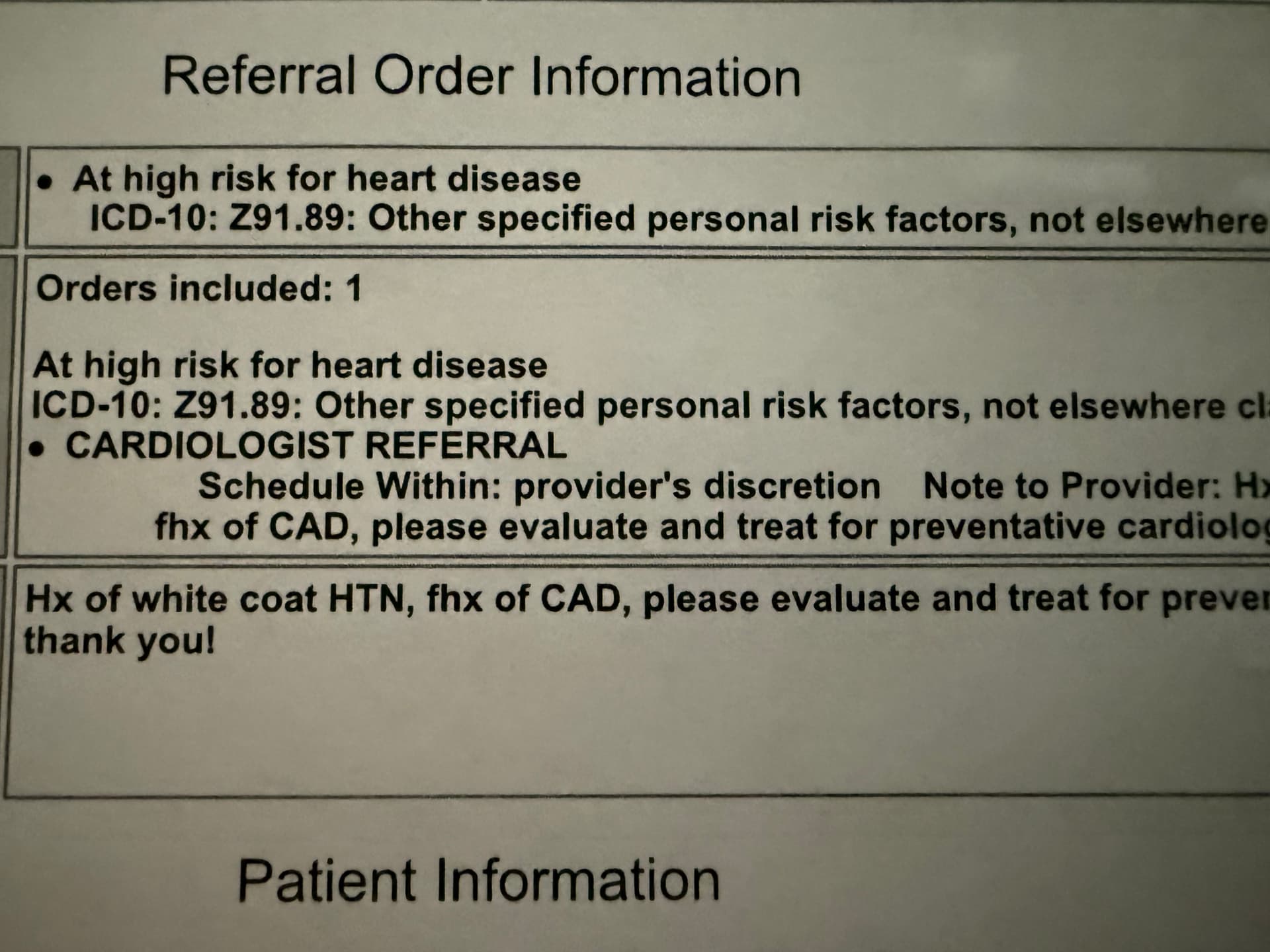
My current doctor (PCP) wrote this on the referral to a cardiologist. Apparently he thinks that my BP is always higher when taken in the examination room than when taken at home. And it is indeed always higher there! Last week while I was at the cardiologist, the nurse took my BP and it was 160/85, meanwhile I had taken it at home an hour earlier and it was 135/75 or something like that, and I showed the nurse my measurement on my phone in the health app. About 3 minutes later, the nurse took it again and it was 140/78.
2 Likes
Same here. If I take my BP at home, it’s usually something like 125/75. At the doctor’s office, 145/80 or so. I blame it on the traffic getting to the office.
intercst
So get to the office 20 minutes early. I have a little bit that helps me zone out, in a few seconds. I end up with a pretty good BP reading. 110/64 at the office last march. Not bad for a crusty of phart of 71.
Steve
I’ve provided enough documentation over the years that they now rarely ask about my BP.
If you’re BP is really 125/75 and they try to reduce it by 10 to 20 points, you’re at risk of falling over from having too low a BP.
intercst
2 Likes
That happened to me once. I did some yoga-style deep breathing for a minute and it dropped back down.
Wendy
The thing to be aware of, though, is that so called “White Coat Hypertension” isn’t necessarily a totally irrelevant finding. The reason that a high reading is noteworthy is that a good many patients don’t have that issue … however stressed they are when they walk into their doctor’s office. What it tells you is that, for whatever reason, there are possibly periods during the day or under certain circumstances, your blood pressure is higher than normal…which obviously isn’t a good thing. Granted, it’s chronically elevated blood pressure that produces the real pathology but sudden spikes against a background of “normal” are probably what causes a good percentage of unexpected strokes.
Edit: to put it in perspective. Apart from the difference in pathophysiology, White Coat Hypertension has a similarity to “prediabetes” in that it’s a measure of some degree of departure from healthy homeostasis. In addition to the increased chance of progression to full blown disease if ignored, this “pre” state quite likely causes some pathological change all by itself.
Here you go…had a quick squint at what was easily accessed on Google. A Harvard publication too…gua-RON-teed to raise the BP of those who have a burr up their bottie over that institution
Not in my case. My new doc is less than a mile away. I could walk there, but there’s a big road between here and there, so I usually drive. Ironically, when I started with my former doc 30 years ago, he was in the same location (different building, but same plaza), but about 20 years ago he moved his office to be closer to a hospital. And recently, sadly, he retired.
It’s not funny! My grandfather died of a too low blood pressure.
That is the case for me. My BP in the morning is higher than the afternoon which is higher than the evening. So in the morning it could be 140/80, in the afternoon 130/75, and in the evening 125/70. I’ll take it now just to see … it’s 122/67 now (11:16pm).

The other good thing about taking it myself is that I do it uniformly EVERY SINGLE TIME. At the docs offices, they use left arm, right arm, elevated, not elevated, etc. I take it with left arm ONLY, elevated and resting on a surface at heart level, seated with feet on ground. And I do that every time, the same way exactly every time. Even when my left arm was in a sling for 6 weeks, I tried to do it as uniformly as possible.
And
Well said.
![]()
ralph