I think the data show that prescription medication is probably a very significant contributor to the opioid addiction problem. For example, in a survey of patients receiving prescription opioids for cardiac implants, 12% developed persistent long-term opioid use behavior.
A study reported in JAMA found that in Tennessee, a whopping 1/3 of the population filled an opioid prescription in the period from 2007-2011. Not surprisingly this was associated with an increase in addiction and overdose.
The British Medical Journal in an editorial noted that in 2015, 240 million opioid prescriptions were dispensed. That’s about one for every American. The editorial claimed that physician overprescribing opioids is a major contributor to the addiction epidemic.
Nah the death count was there. No conjuring up anything. Yes the regs were there all along. The pharmacies made money by ignoring the rules. They just lost in court because they ignored the rules. Not sure what you are trying to say.
It would be a mistake to infer from the snippet you’ve posted that I’m in any way denying the association between access to and subsequent abuse of prescription pain meds. Manifestly, if the abused substance of choice is only a drug that can be obtained by prescription alone then, by definition, a prescription is the source (legally obtained or not). You don’t need to do a tremendous amount of reading around the topic to see that the addiction/overdose epidemic is a little more complex.
To your links…
I discounted your BMJ article as a worthwhile source. This was an opinion piece, basically and the apparently damning statement implying that whilst some surgeons prescribed opioid pain meds judiciously (presumably Makary’s team?) others send their patients home with a swag of weeks and weeks worth of highly addictive stuff. No way to check whether this was fact or opinion as the paywall kicked in.
The JAMA study doesn’t really tell us much that we dont know now in 2022 based as it was on data mined over a period 20 or so years ago…and with many of the references that either predate the study period or were opinion pieces in non peer publications. I didn’t have the stamina to wade through it to confirm an already established fact that excess prescriptions can be tracked closely.
Your press release…although it was a press release and subject to the usual issue of the banner headlines not quite representing what the study actually tells us. This ended up being an interesting read …the primary document, that is. The actual movie…not the report based on the trailer. Here’s the link…
I guess there are a number of ways to interpret any study and this is as good an example of any. Now, it might be me misreading your statement here, but it looks on first blush as if you’re confusing the authors’ use of persistent opioid use (POU) with the opioid addiction problem…and that might very well be the authors’ opening statement because that’s how it looks. Initially.
Now, this was a new term to me (POU)…but per the authors’ definition, this term meant a second prescription within 30 or so days of their first post op prescription and not a descent into a life of addiction. These data were obtained from a prescription database, BTW, not patients’ survey (always iffy) so likely a true representation. Here’s the thing, though…they also appear to have standardised the different prescriptions for dosage by something called oral morphine equivalent (OME) and, unless my math is dodgy, the two prescriptions combined were a bit less than the orthopod gave me as ostensibly a one time only script. Blimey, if I’d have asked for the top up meds I really needed I would’ve been considered a persistent opioid user. So, without any understanding of the need WRT the procedures and follow-up care, this doesn’t look to me to be a major contributor to the opioid epidemic but rather an example of judicious prescription of opioids.
Another interesting feature of this study is that there are hyperlinks to other articles. One statement that was a eye opener is that, prior to the increase in use of opioids in the 1990s, the US was already using 80% of the World’s opioid production. Still got more to plow through so I thank you for the edutainment.
My position is that overprescription of opioids in the early 2000s, particularly oxycontin, was a significant, if not primary, driver of the current opioid addiction epidemic. I think the numbers bear that out. When a third of a state’s population filled an opioid prescription over a five year period and the US had 240M opioid prescriptions in a single year, I think it obvious that there was a problem.
The US judicial system apparently agrees with me given legal judgements against manufacturers and distributors for their actions during that time period. The CDC also seems to agree as they felt the necessity to issue guidelines in about 2016 that asked doctors to be much more judicious in prescribing opioids. There were still 140M opioid prescriptions in 2020 for the US, a big decline from 2015 but still a remarkably big number. Just as a comparison, according to the CDC in 2020 there were 202M oral antibiotic prescriptions. It is astounding to me that opioid prescriptions are in the same ball park as antibiotics.
Unfortunately the decline in opioid prescriptions was a bit late as the increasing addiction numbers over the last decade or two stimulated the expansion of a black market for drugs like heroin and fentanyl.
So what part of this narrative do you think is incorrect?
No problem. Keep in mind that much of the original studies are behind paywalls. I have access to these but most here don’t so there isn’t much point to link them. That means that confirmation here is largely limited to links to popular media.
No problem. Keep in mind that much of the original studies are behind paywalls. I have access to these but most here don’t so there isn’t much point to link them. That means that confirmation here is largely limited to links to popular media.
I think it’s a given that if you’re looking for confirmation of any belief, search engine algorithms ensure that you’ll find nothing but, right? It’d be the same if you typed, say, “MMR vaccines and autism” into Google.
Thing is though, the posted link that looked most damning and would’ve gone a long way to refute my contention … that very few folk run a risk of descending into a life of drug abuse and addiction from a first encoubter with legitimately prescribed opioids (this presupposes, of course, no history of other substance abuse) … did have a link to the primary document. So, even though the article you posted and the opening comments in the study itself appeared to imply that 12% of patients receiving opioids following a cardiac procedure developed an abuse disorder, it became very apparent that this was a gross misrepresentation.
On looking at the statistics provided, of the demographic studied only 11% of patients used the initial prescription (for something like 18 x 5 mg oxy) and of that already small number, 12% required a second prescription…which is hardly surprising seeing how few tablets were originally prescribed. I don’t know how painful the procedure was, but I’d be pretty miffed if I found myself branded as a drug seeker just because I didn’t like pain.
You are leaving out one vital piece of information. Persistent opioid use is defined as a second prescription at least one month after the surgery. The assumption is that the pain for a relatively minor surgery should have subsided by then. As for the small numbers, that actually supports my position. The surgery is sufficiently minor that only a small number require opioid pain killers. Of that small number, 12% are still using opioids at least one month after the surgery.
This led an author of the linked paper to conclude:
“Even a small number of oxycodones can start the addiction process,” said senior author David S. Frankel, MD, an associate professor of Cardiovascular Medicine and director of the Cardiac Electrophysiology Fellowship Program at Penn. “The significance of this study is to make other electrophysiologists aware that even a low-risk procedure like a pacemaker or a defibrillator can lead to chronic opioid use and that physicians may want to be more conservative in prescribing opioids after surgery.”
In another study of persistent opioid use (now given the more stringent standard of use at least 90 days after the surgery) similar results were obtained. The conclusion of the authors:
“In a cohort of previously opioid-naive patients, approximately 6% continued to use opioids more than 3 months after their surgery, and as such, prolonged opioid use can be deemed the most common postsurgical complication. New persistent opioid use is not different among patients who underwent minor and major surgical procedures, thereby suggesting that prolonged opioid use is not entirely due to surgical pain.”
I guess you could continue to argue that persistent opioid use has nothing to do with addiction but I think that is basically sticking your head in the sand.
During my bilateral mastectomy in 2015 for double-sided breast cancer, I had expanders implanted under my pectoral muscles to stretch them to accept silicone breast implants. The expanders were rock-hard and painful. The process went on for months before the expanders were swapped for the soft silicone implants.
I took opioid painkillers for two months since my pain was very bad. This wasn’t due to addiction. My experience is that opioids aren’t addictive as long as they don’t make you feel good but only take the edge off severe pain (together with NSAIDs and acetaminophen at the same time).
Don’t say that this is “sticking your head in the sand” until you, personally, have severe, intractable pain. Which you probably can’t imagine until it happens to you.
Wendy
The thing that opioid naive people don’t understand is that, pain relief aside, opioids aren’t pleasant drugs to take. They make you feel a bit “dopey”, nauseous and they cork you up like nobody’s business. Back when I had the practice, when double checking a new patient’s medical history I noticed quite frequently that second only to an allergic response to penicillin was codeine/Vicodin/the percs. etc. Now, given that it’s important to double check a claimed allergy (even to the Usual Suspects like antibiotics) I’d always ask how this “allergy” manifest itself. Disorientation, nausea and constipation were the responses. When I’d point out that these were normal side effects of the drugs, I swear they’d look at me as if I was crazy…because, how do people get addicted to anything that does that???
P.S…mind you, both our outcomes might’ve been different if we’d been tobacco users, suffered from alcohol and other substance abuse disorder, mood disorder or any of the other risk factors itemised on the posted link.
You certainly have my sympathy and respect for your experience but I would gently suggest that what you went through was probably not the norm for the 240M opioid prescriptions fulfilled in 2015. Opioid pain killers are obviously a necessary component in the treatment of pain. It certainly was for you. But that is a separate issue from whether it was overprescribed and if that overprescription is the cause for the current opioid addiction epidemic.
To be clear, are you and VeeEnn arguing that the high levels of opioid prescriptions beginning in about 2000, and in particular the marketing and availability of Oxycontin/oxycondone were not major contributors to the rise in opioid addiction levels that occurred during that same time period?
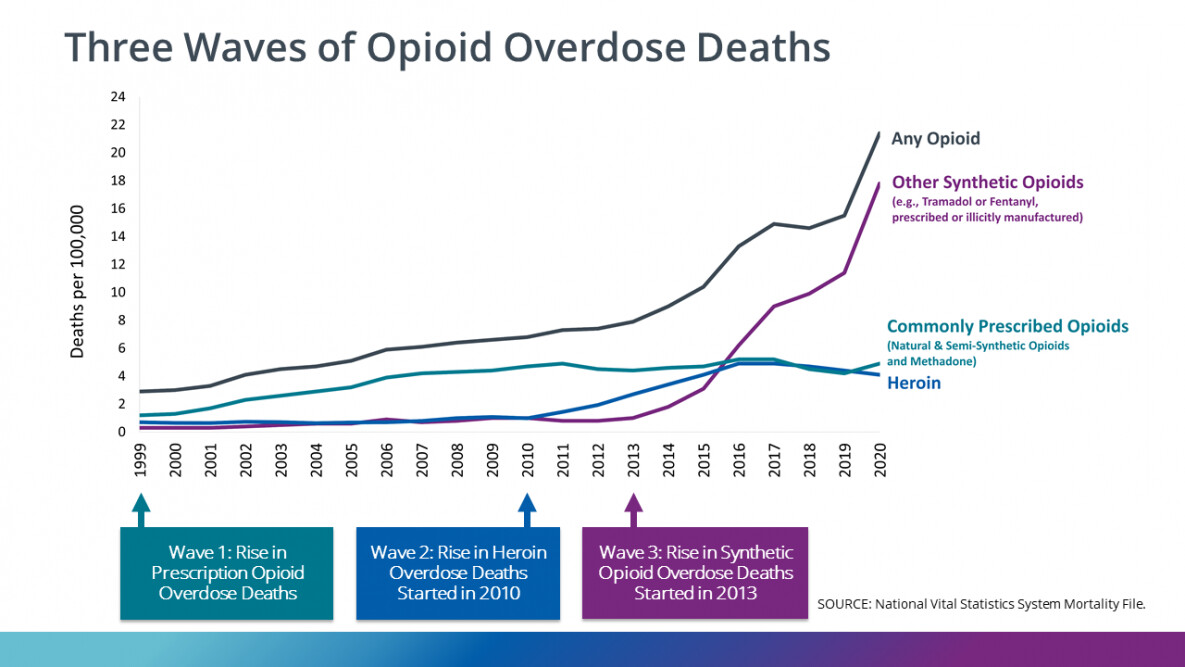
The CDC has a graph depicting the rise of opioid overdose deaths in America. The increase began in 2000 with opioid prescription overdoses. This was followed by the uptick in heroin in 2010 and synthetics in 2013. The likely foundational role of overprescription of opioids to the current opioid addiction epidemic seems pretty obvious.
I agree the hammer of regs is hitting more than the nail on the head. People with major pain problems need the care.
The inactions concerning the abusive use of opioids had or has to be stopped. The major companies profiting off of it would kill my family member, your family member or anyone’s for a buck. That is very wrong.
The law swang to far the other way. Patients do need painkillers. That is no reason to side step the addiction problem. Doctors are overachievers it is getting straightened out. The drag is the bureaucracy.
I won’t answer for Wendy but what I have been saying is that a legitimate prescription for an opioid painkiller is not likely to pitch a person who doesn’t already have substance abuse issues into an addiction spiral
For sure, more opioids in circulation makes it much easier for folk who wish to use them for recreational purposes to get a hold of them so, manifestly here’s a potential for more opioid abuse. Availability offers more temptation to the existing or potential addict.
OxyContin presented its own unique issues when it hit the market. For anyone not totally familiar with this formulation, it was a specially coated time release form of oxycodone. Intended to even out the highs and lows of the more readily metabolised form as an attempt to reduce the potential for dependence and addiction with long term users (not opioid naive, for obvious reasons). A plausible mechanism of action, it seems, if taken orally as prescribed. Thing is, addicts getting a hold of the stuff didn’t take it as Intended but either chewed, crushed and snorted, injected or even shoved it up their bum!!! In the process, getting a super high the likes of which were apparently not available with abusing regular oxy. Not something any manufacturer should be held accountable for, in my opinion. Problem was, it transpired that even the proper formulation still had the same addiction potential and Perdue had hidden the data, misleading an inadequately diligent FDA as well as the doctors it was marketed to.
Another issue muddying the waters is the unintended consequences of the rehab/recovery industry. Something I’d never thought about until a former user wised me up.
After a stint in rehab and getting “clean” a good many folk go back to using (I’m sure the intention was there to stay clean but sometimes the underlying problems don’t disappear) …oftentimes at the same amount of drug as before and not realising that the tolerance they’d built up over the months/years of abuse had diminished. A former “just right” dose is suddenly an overdose.
You can learn a lot from drug addicts…and find out that they are generally not like you.
ah but that is so untrue. There were a lot of high school student athletes who needed a painkiller and became an addict as the doctors were misinformed early on about opioids. Today most of those kids would have been sent home with Tylenol. Many of them either have shattered lives or lie dead.
There were also a lot of high school students that were not addicts but young and trying drugs experimentally. I know of one who was drinking on graduation night and popped one Oxy. His mother came down stairs the next morning and found him dead. He was not an addict just young.
Meanwhile, we have luminaries like a Councilman in Middletown, Ohio, and the Sheriff in Butler County, Ohio who advocate refusing to administer Narcan to addicts, and letting them die, as the Puritanical punishment culture raises it’s head again.
The rise of opioid addiction and other “deaths of despair” (alcoholism and suicide) are clearly related to macroeconomic factors – the loss of well-paid factory jobs in middle America that began in the 1980s and accelerated in the 2000s. The chart of manufacturing employment correlates closely with the rise in opioid overdose deaths (negative correlation).
It’s no coincidence that lower back pain, which has no objective measure for diagnosis, is the largest source of disability in the U.S. It’s no coincidence that laid-off workers can go to a doctor and get on Social Security Disability but ONLY if their back pain is disabling enough that they cannot work at any job – so severe that they need opioids to treat it. It’s no coincidence that these despairing laid-off workers, with no hope of regaining the American dream that was snatched away by outsourcing, are dying from overdoses.
A book has been written about this: " Deaths of Despair and the Future of Capitalism," by Anne Case and Angus Deaton.
The medical pendulum swung from ignoring pain* to treating pain as a vital sign which needs to be aggressively treated to withdrawing painkillers even from surgical and cancer patients in dire agony to (hopefully) a balanced approach to pain control.
The agony caused by macroeconomic despair is real but it should not be treated by opioids. Doctors need to treat actual physical pain adequately while withholding addictive opioids from those whose pain is more existential than physical.
Wendy
I can personally attest to doctors’ ignoring pain since I was subjected to two (2) bone marrow taps without anesthesia at age 16 in one day. (1970) Each bone marrow tap consisted of a doctor hammering a large-diameter hypodermic needle into the top of my hip bone with a mallet. This was pure torture. They failed to get an adequate sample the first time and returned a couple of hours later to repeat the biopsy on the other side. The pain lasted for hours after the test but I received no medication for it. Fortunately, this test is now done with anesthesia.
A fair number of opioid overdoses involve other drugs…alcohol being at or near top of the list. Opioids, among their other properties, are respiratory depressants so add ethanol… As to whether just one could do it, well, theoretically possible. If you’ve drunk enough that you’re so close to the edge, one could do it and kick in sometime later and render a person unresponsive to, say vomiting from the volume of alcohol drunk.
I guess that’s how binge drinking at frat parties happens…just that one extra measure of alcohol on top of everything else can be the difference between a drunk with a hangover or a corpse. Would you blame the last drink (or one oxycodone)…or the sum total of ethanol?
If you are getting drunk that is a depressant. Having an oxy on top of that I think, it has been a while since I heard this, slows the heart till it stops. I believe Oxy is another depressant. He came in after all the partying turned on the TV and sat down. His heart stopped. His mother found him in front of the TV the next morning.